Military Vaccine Mandate Part 1.
Military Vaccine Mandate Part 1.
Are service members being affected at an equal to worse off than the general population?
*The writings, thoughts and opinions here in are the authors own and represent in no way any organization, group, or service that the author may or may not be a party to. To include any state, federal, or non government entity*
“It quickly becomes apparent by looking at very simple data that decision-makers, both military and civilian, have no real good reason for the mandate, outside of getting in line as not to be cast out of the church of “THE” science.“
09 August 2021, Secretary of Defense Austin Announces COVID vaccine mandate. To most service members it didn’t come as a surprise, being forced to get a vaccine is commonplace. Regardless, service members, in not insignificant numbers, are still asking “Why?” I found myself asking too, “Why?” After far too many failed attempts at getting a cogent answer out of anyone in charge other than “it is safe and effective”, I decided to look into it myself.
To preface this, I took the general age of military personnel 18-49 and used that as my comparison tool against the general public. This is the age group that public health researchers have been using, constitutes the majority of our force, and results would not be skewed by children who are barely affected and the elderly who are substantially more affected.
The first question examined was, “are service members being affected at an equal to worse off than the general population” This is an FDA “approved” experimental drug, as stage 3 trials are being conducted by the governments of the world until 2023, so there had to be a reason this drug was being mandated to one of the healthiest subsets of the country. To explore that I wanted to look at whether or not the military was being infected, thus missing work and affecting mission readiness, at a higher or equal rate observed in the general population, i.e. hospitalizations and severe illness.
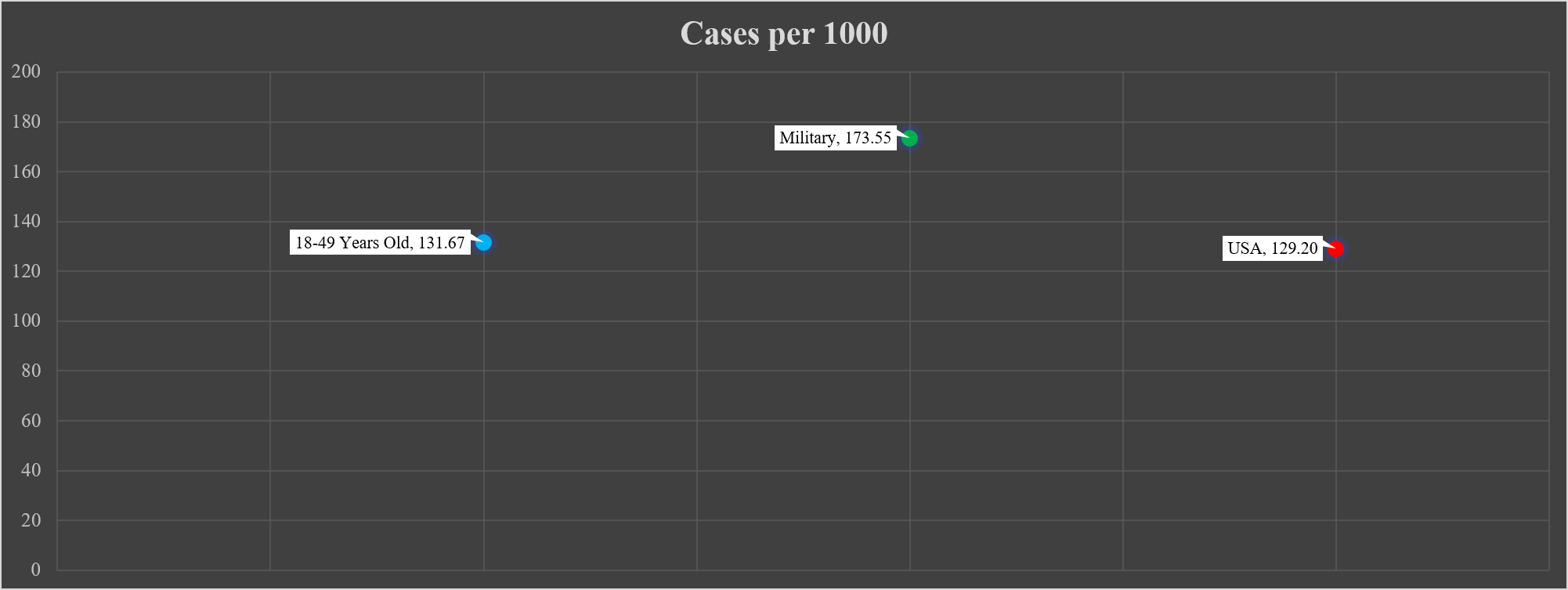
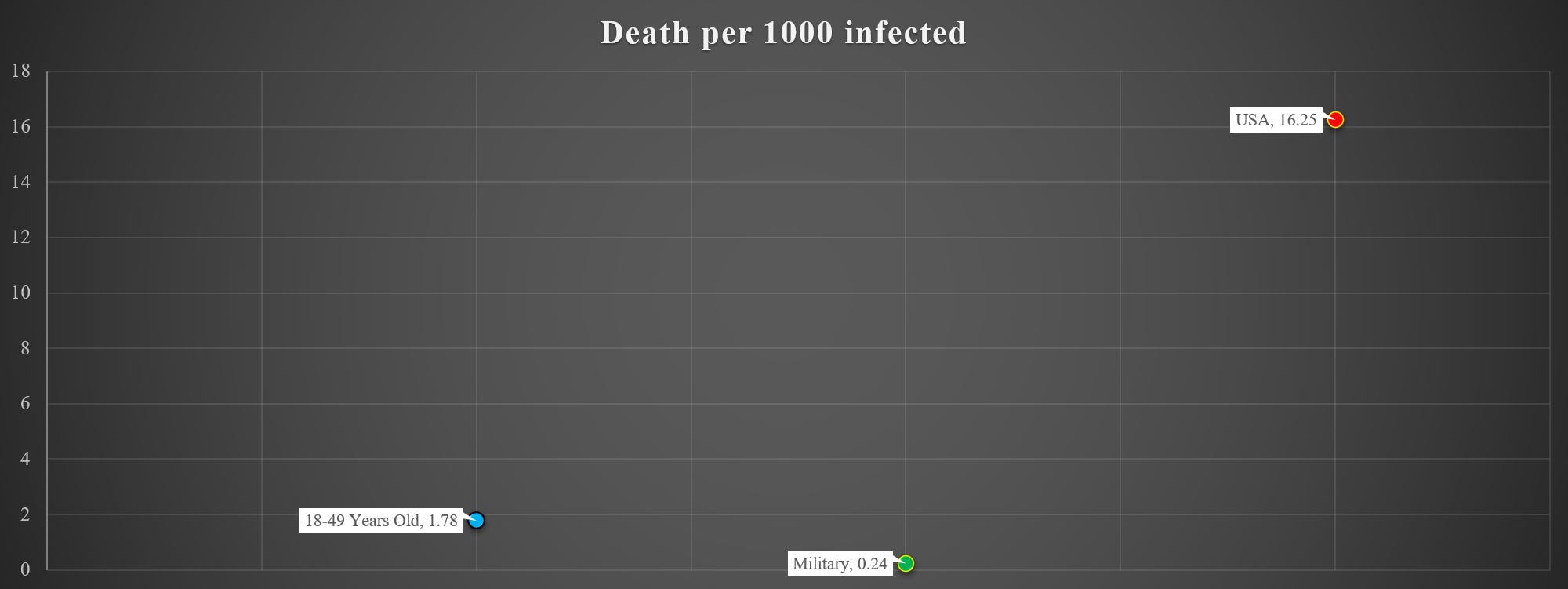
What I found was that military members were getting infected at a higher rate than the general population, which was not particularly surprising for a multitude of reasons. The military case rate, while 14% higher than the civilian population, must be put in context. Military cases constitute 0.57% of total US COVID cases while having infected 17% of the total force. And while the military’s case per 1000 rate is higher than the general 18-49 year old public, the military is more than 8 times less likely to die when compared to the equivalent general population, a 733% decrease. While the 18-49 year old civilian population has almost 2 per 1000 people dying, the military is sitting at .24 per 1000, or 1 in around 4000.1 2 3 4
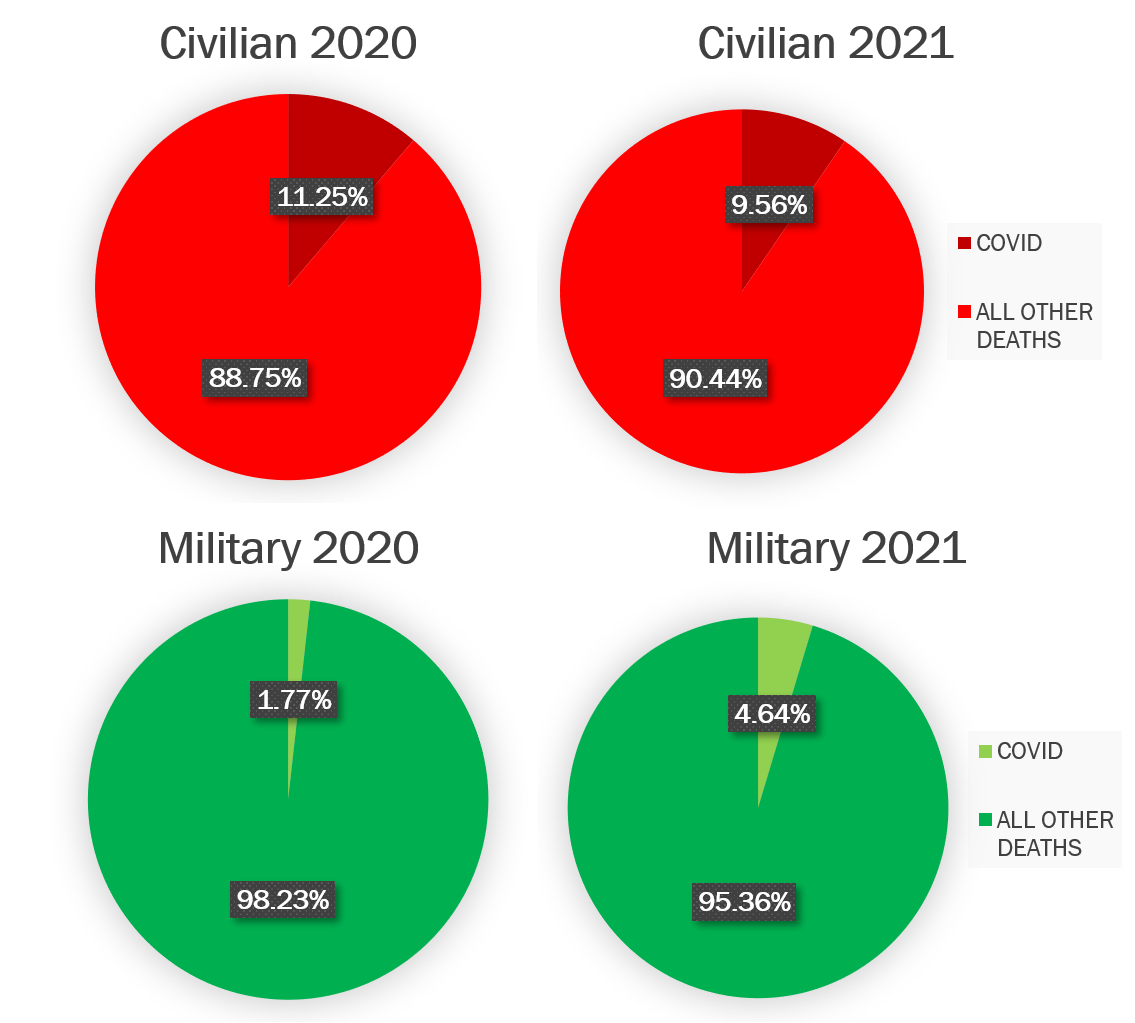
Not only are military members not dying at the same rate when infected, but even though the military has a higher proportion of infected individuals, 17% military to 13% civilian, military members have had 0.0041% of their population die during this pandemic while the 18-49 year old’s sit at 0.023%.5 Both of these numbers are extraordinarily low for as drastic of steps as have been taken such as mandating comparatively untested medications, based on observational data and emotion-driven decision-making processes.
Hospitals overflowing was one of the principal concerns at the beginning of the pandemic, “Flattening the Curve” and such, but I was unable to find convincing data showing that the military while being infected at a higher rate, were contributing in the least to any hospital burdening. Now, this does not take into account localized outbreaks, but with numbers as low as having been observed, it doesn’t make sense to assume military members would even moderately contribute to overburdening the healthcare system.
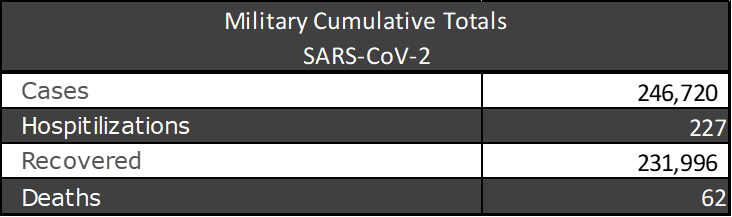
Based on the known data, 18-49 year old’s have been hospitalized a total of 6,000,000-12,000,000 times.67 Military members, who we have exact data on, have been hospitalized in just 1% of their cases and only 0.16% of the force has been hospitalized. This without immunization, most members doing little to nothing to guard against the virus such as masking or social distancing, and in many states living overall normal lives.
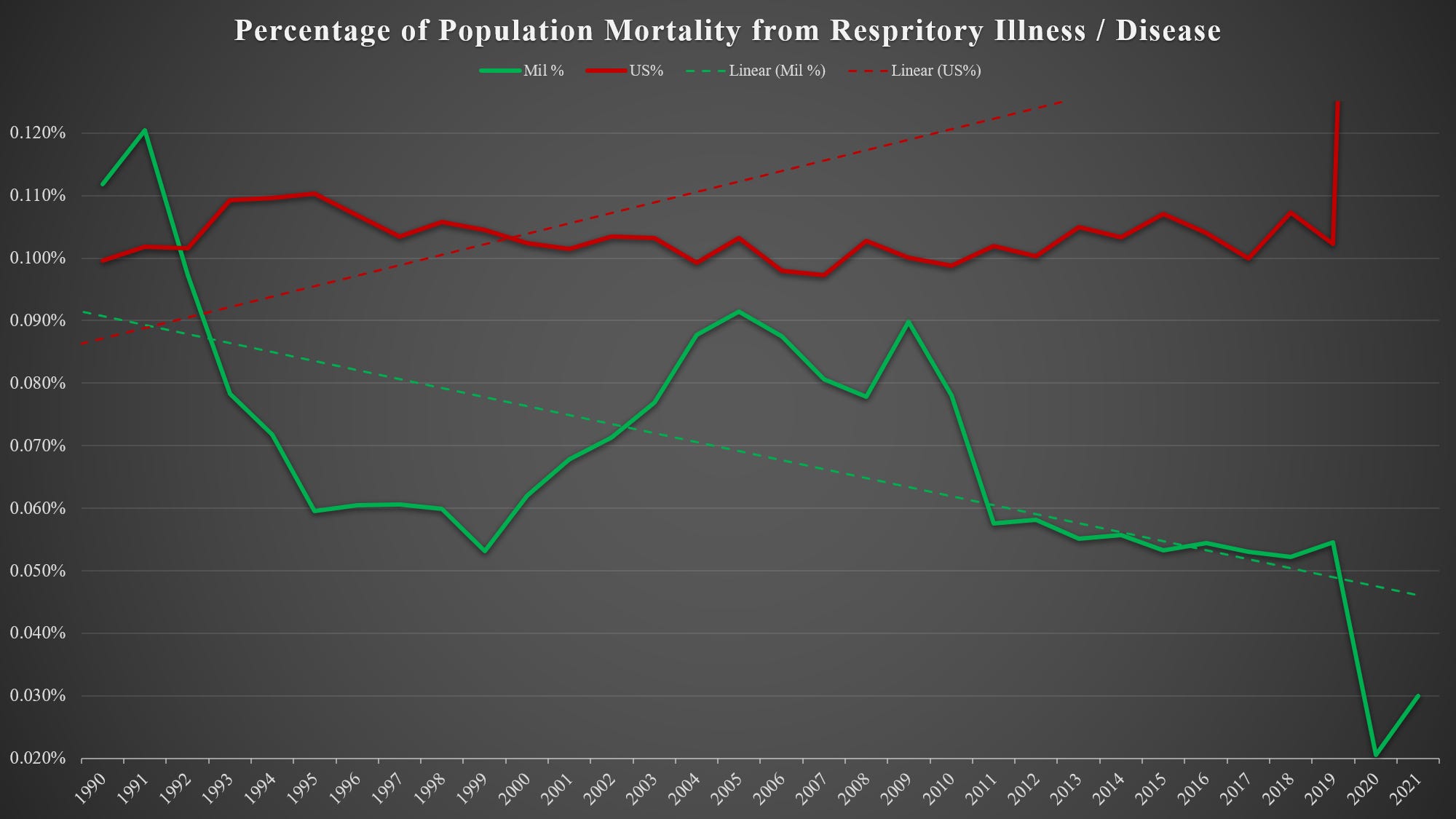
So if members aren’t getting seriously ill very often and going to the hospital, and they aren’t dying at an even liberally comparable rate, then this virus must be a massive departure from year-to-year outcomes. Well, that too does not seem to be the case. Luckily, the military keeps very detailed records when you die, the CDC and FDA do as well so extrapolating that information out wasn’t too difficult and would have been quite simple for policymakers to do themselves.
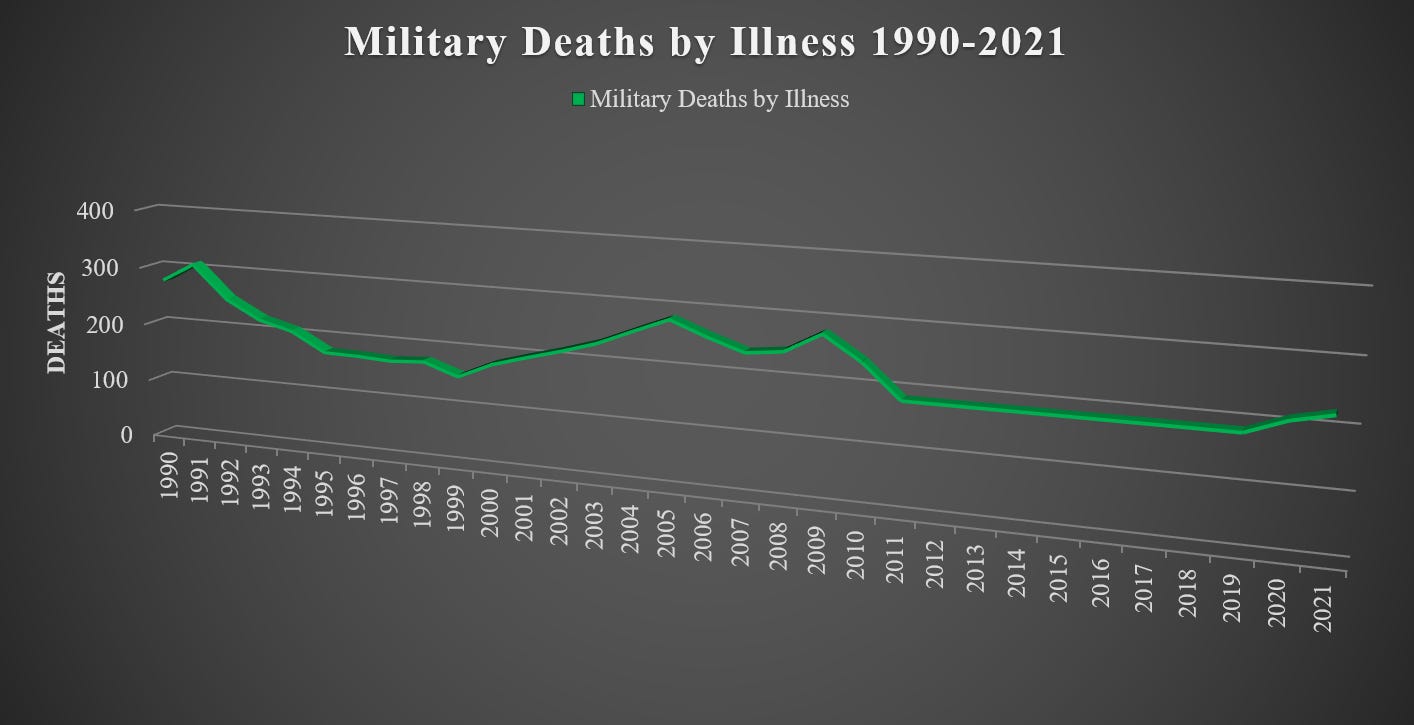
Based on 31 years of data, from 1990-2021, there were 29,898 military deaths, of which 6,794 were from illness, equaling roughly 23% of service member deaths in that period. We can look at the years without COVID and see if there are any comparisons to be had, turns out there are.8 From 1990 to 2019, we lost 0.4%, less than half of a percent, of military members to illness or disease and it accounted for 18% of all deaths. Unfortunately, when factoring in 2020/2021 we saw those numbers, well, not do anything unless we want to start counting in 100th’s of less than one percent. When looking at the years individually you do see a higher jump, up into 22% and 24% of deaths respectively, but as far as total threat to force goes there is no real change, certainty not warranting anything near statistical significance.
It quickly becomes apparent by looking at very simple data that decision-makers, both military and civilian, have no real good reason for the mandate, outside of getting in line as not to be cast out of the church of “THE” science. It is concerning not only that military decisions are being made through a civilian lens, but equally disturbing why it is being done.
Were the military made up of people of the age of, oh let's say, Joe Biden, absolutely there should be mandated shots. Unfortunately, we aren’t quite that old. To put the risk assessment for 80-year-olds with everyone, ESPECIALLY the people you have to call on to fight your wars, without knowing ANY long-term side effects is criminally moronic. The priests of this new religion will surely disagree with all of the above so let's look now at the vaccine.
“Provisional Deaths by Age and Sex Data.” Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. Accessed October 12, 2021. https://data.cdc.gov/d/9bhg-hcku/visualization.
“CDC Covid Data Tracker Demographics.” Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. Accessed October 12, 2021. https://covid.cdc.gov/covid-data-tracker/#demographics.
“CDC Wonder.” Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. Accessed October 12, 2021. https://wonder.cdc.gov/.
Elflein, John. “Total Number of COVID-19 Cases by Age U.S. 2021.” Statista, October 8, 2021. https://www.statista.com/statistics/1254271/us-total-number-of-covid-cases-by-age-group/.
“Two More US Service Members Die from Covid-19, Bringing Military Deaths to 17.” American Military News, January 22, 2021. https://americanmilitarynews.com/2021/01/2-more-us-service-members-die-from-covid-19-bringing-military-deaths-to-17/.
18-49 age range used due to public health reporting. CDC and WHO data for cases and hospitalizations based on estimates with 95% UI*
“Coronavirus: Dod Response,” U.S. Department of Defense, accessed October 12, 2021, https://www.defense.gov/Spotlights/Coronavirus-DoD-Response/.
“Trends in Active-Duty Military Deaths since 2006.” Federation of American Scientists. Congressional Research Service. Accessed October 12, 2021. https://sgp.fas.org/crs/natsec/IF10899.pdf.