
Military Vaccine Mandate Part 4.
Military Vaccine Mandate Part 4.
We are putting our forces at an arguably greater risk than if all members were to get COVID.
*The writings, thoughts and opinions here in are the authors own and represent in no way any organization, group, or service that the author may or may not be a party to. To include any state, federal, or non government entity*
“Bottom line, there is NOT enough yet known about long-term effects, service members do not need vaccination, and the estimate of just cardiac adverse drug reactions is orders if magnitude higher PER shot. With inevitable boosters, we are exponentially INCREASING our risk to the force while our risk to the force from the virus, that, due to multiple variables NOT including the vaccine, is DECREASING.”


After looking at to supposed benefits of the vaccine, we need to look at the safety of the vaccine. Surprisingly after losing lawsuits due to the anthrax vaccine, the DOD is going ahead with where the political tide is taking them and there isn’t data to support the safety of this vaccine.
First and foremost, there are no longitudinal studies done on this drug, other than observational data being done on the world population as we go forward in time. We have absolutely no idea, even if the chance is low, what this could do to people. Say it has around a 0.0251% chance of killing people over time, like COVID for the military, should that not be taken as seriously? For that percentage point, we have masked people, not let them go to work, and threatened to fire them. So shouldn’t mandatory vaccination, have a similar, if not higher since this is by choice of administrators and “leaders” risk aversion due to liability? I mean the class action, if something does happen, is more negligible than the number of campaign dollars one would have to spend to dig themselves out of the “anti-vaxxer” hole, but don’t we owe our service members that?
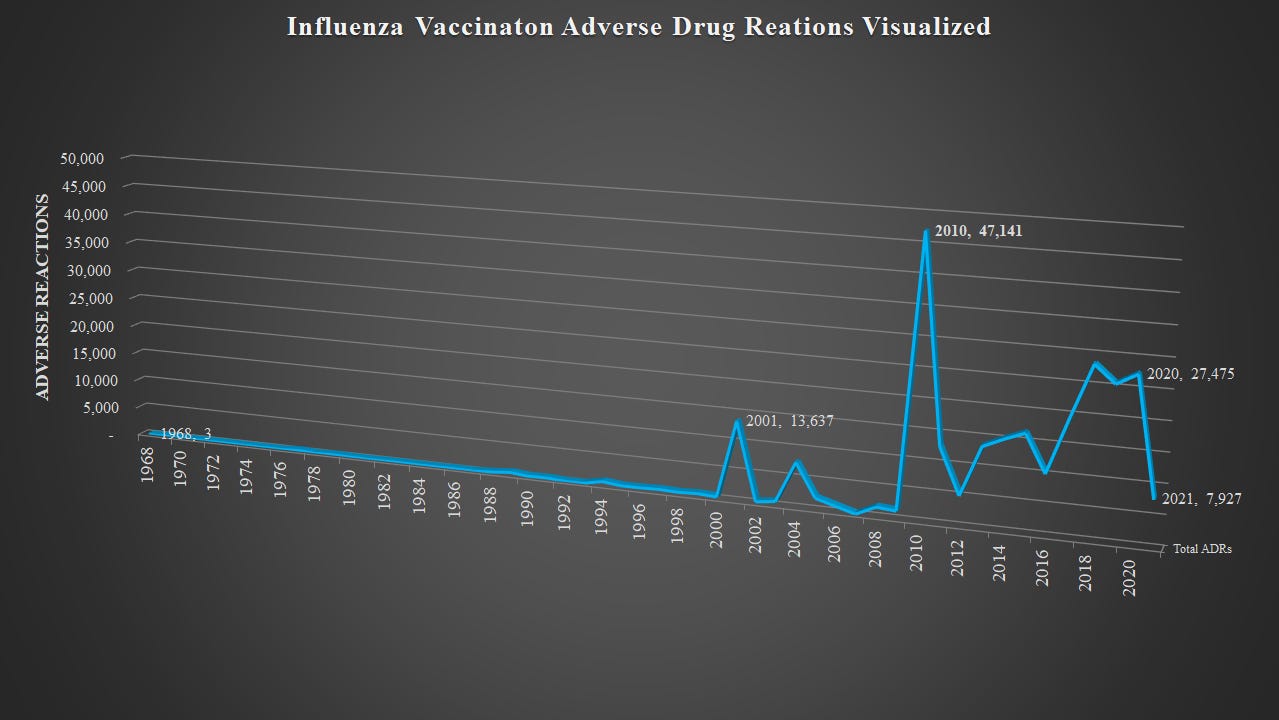
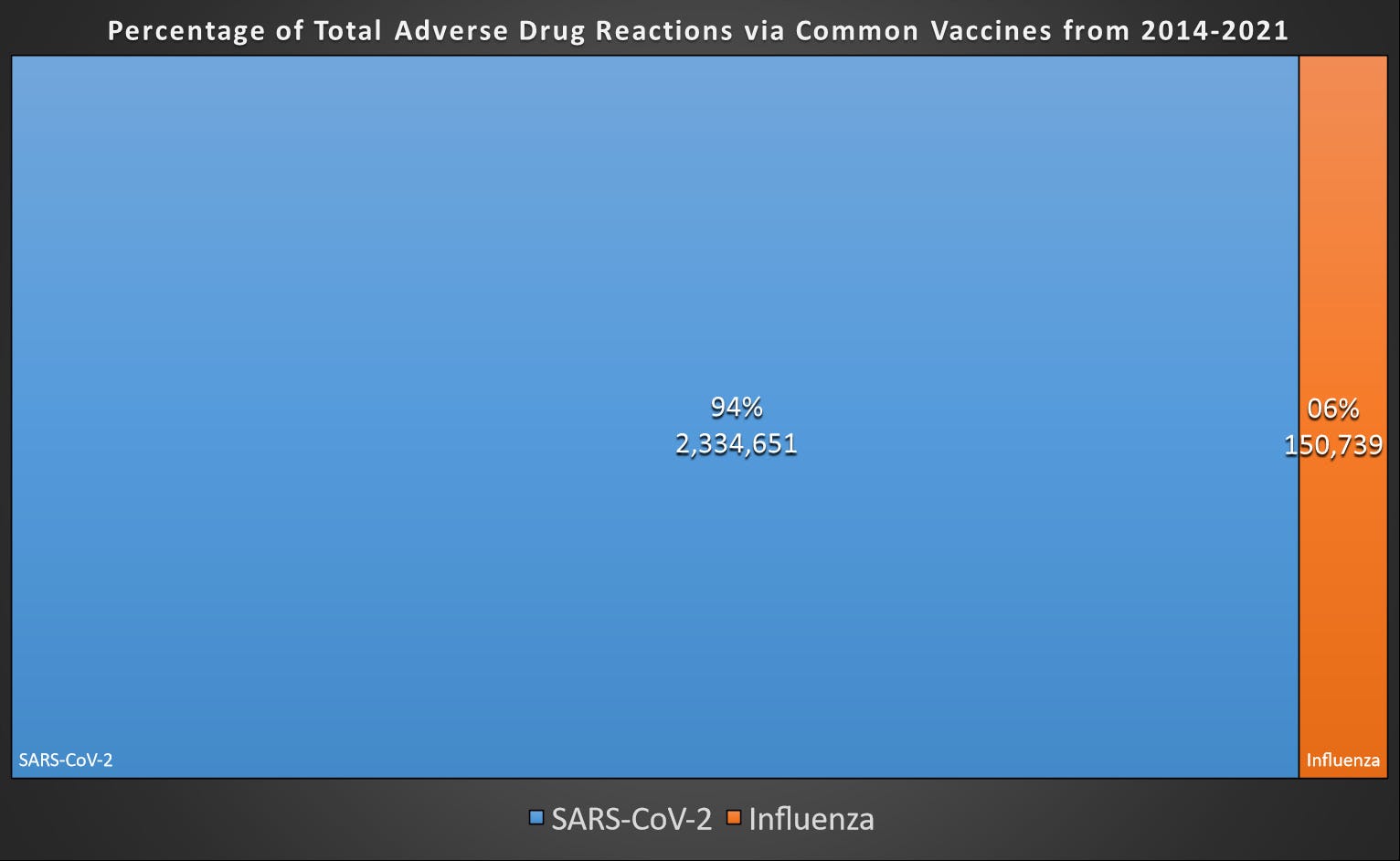
Using a joint WHO-Uppsala system called “Vigiaccess” we can see how many ADR’s (adverse drug reactions) any particular drug has had. Above is the table that is produced when looking up Comirnaty. One might see that and think, oh that’s just because we have given SO many vaccines these last 2 years, which we have, but you can easily compare it to a drug that is supposed to do something similar and has a much longer period to look at. One such drug would be the influenza vaccines. By taking ADRs on the influenza vaccine and the mRNA vaccine Comirnaty, we can EASILY see this isn’t the same.
By comparing the two vaccines, we can see that even though we have been inoculating people all over the world with influenza vaccines, between the two COVID vaccines constitute 94% in just ONE year of all adverse drug reactions when you adjust for the time since the very first use of an mRNA vaccine was used. This isn’t a result of dialing in the influenza vaccine either, below we can see that the influenza vaccines are pretty steady throughout their entire life of use.1

Based on very simple to attain numbers, in almost 2 years we have a 781% INCREASE in ADR’s and all military members are being told is “they are FDA approved, safe and effective”.
No, that isn’t good enough. This needs to be explained and accounted for before putting the force at this level of risk.
The DOD states they have given over 5,00,000 shots, based on that we can look at the ADR’s we can expect from the vaccinations.2 Part of that is understanding that many ADRs are due to self-reporting, and not clinical data. Some of the ADR’s that are most worrying, like myo/pericarditis are generally clinically indicated and an individual may not know that is happening to them. I fully acknowledge that many of the adverse reactions are not serious illnesses, but it is too soon to tell. Concurrently we have a virus that we DO know plenty about. To bolster that, even the CDC director is acknowledging, which is backed by data, that the vaccines aren’t stopping transmission OR lessening viral load, it brings me back to the original question. WHY?3 might see that and think, oh that’s just because we have given SO many vaccines these last 2 years, which we have, but you can easily compare it to a drug that is supposed to do something similar and has a much longer period to look at. One such drug would be the influenza vaccines. By taking ADRs on the influenza vaccine and the mRNA vaccine Comirnaty, we can EASILY see this isn’t the same. Current known data, again based mainly on under-reported self-reports, show that 1% of shots are producing ADRs. On the next page, just based on that we can estimate the number of service members either knowingly or unknowingly being affected by those adverse reactions.
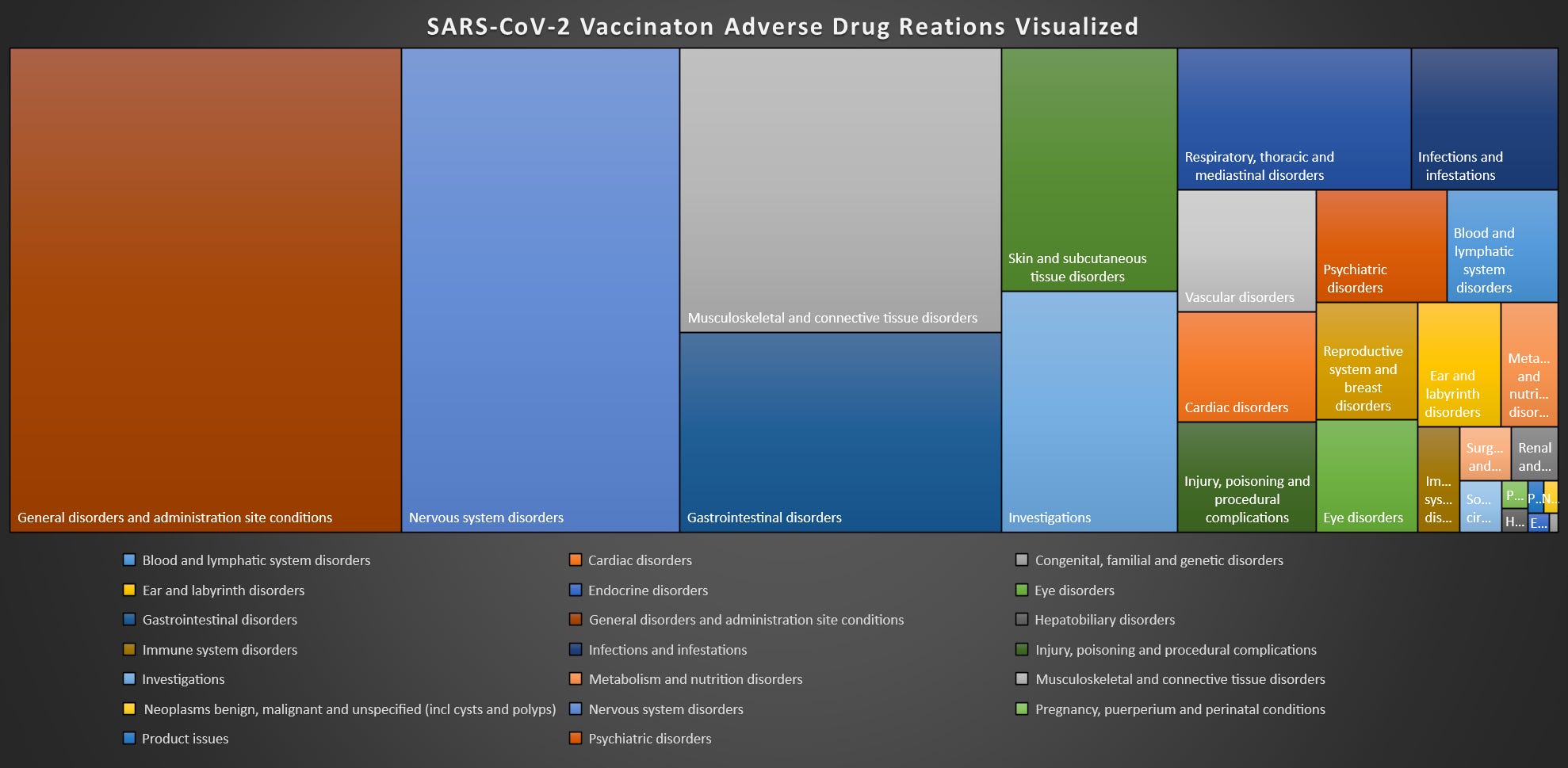

As we can see by the ADR’s indicated in RED, those are adverse reactions that at this point are estimated to be HIGHER than those military members that have died from COVID. While injection site issues aren’t especially worrying, vascular disorders, respiratory, thoracic, and mediastinal disorders, psychiatric disorders (since the military has a GREAT track record with that), connective tissue disorders, nervous system disorders, infections, gastrointestinal disorders, eye/ear disorders, and CARDIAC disorders (ranking 10th out of 28), those are a problem.
And to be clear, this would NOT be as much of a problem were ANY member of the medical, administrative, executive, or military leadership answering questions, acknowledging this is happening and the inverse relationship between members they are forcing this on and the general population, and what the plan is to do if it turns out in 2-10 years these vaccines turn out to do some serious damage to humans, or the people who volunteered to do just about anything for this country. But that contract is based on the trust that those above them aren’t going to run them into a buzz saw.
Bottom line, there is NOT enough yet known about long-term effects, service members do not need vaccination, and the estimate of just cardiac adverse drug reactions is orders of magnitude higher PER shot. Now with the conversation about boosters, we are exponentially INCREASING our risk to the force while our risk to the force from the virus, that, due to multiple variables NOT including the vaccine, is DECREASING.
Full reference list can be viewed in the original post or in the data and references post.
Center for Biologics Evaluation and Research. “Influenza A (H1N1) 2009 Monovalent Vaccines Descriptions, Ingredients.” U.S. Food and Drug Administration. FDA. Accessed October 12, 2021. https://www.fda.gov/vaccines-blood-biologics/vaccines/influenza-h1n1-2009-monovalent-vaccines-descriptions-and-ingredients.
Forgey, Quint. “Pentagon: 70 Percent of Service Members Have Received First Dose of Covid Vaccine.” POLITICO. POLITICO, July 18, 2021. https://www.politico.com/news/2021/07/16/military-coronavirus-vaccine-499822.
“US Centers for Disease Control,” US Centers for Disease Control (CDC, July 30, 2021), https://www.cdc.gov/media/releases/2021/s0730-mmwr-covid-19.html.