
Military Vaccine Mandate Part 3.
Military Vaccine Mandate Part 3.
Data shows, with a high probability, the vaccine will do NOTHING for military personnel and is purely political.
*The writings, thoughts and opinions here in are the authors own and represent in no way any organization, group, or service that the author may or may not be a party to. To include any state, federal, or non government entity*
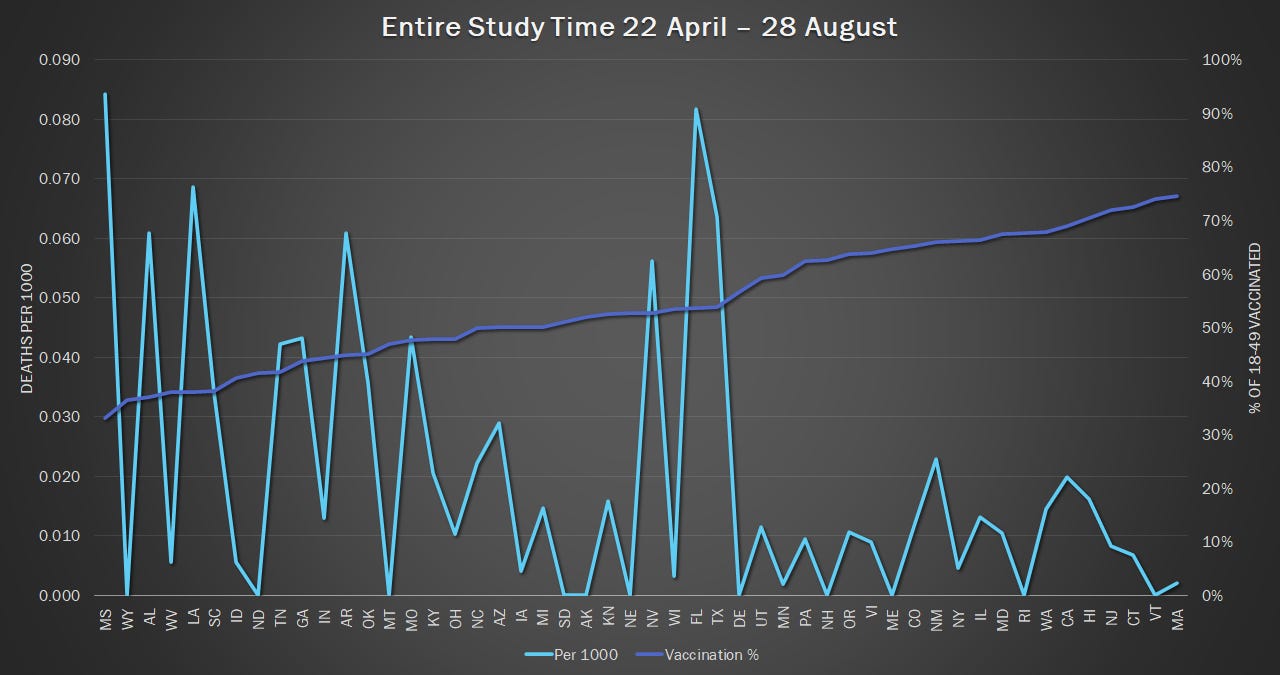
“The key takeaway, a negligible (near non-existent) correlation was observed by higher rates of vaccination in a state and deaths per 1000 over periods.”
What does the data say?
Health agencies have been monitoring COVID pretty heavily, what that gives us are LOTS of numbers. The bad thing about this many “numbers” or data sets, is it is extremely easy for them to become convoluted or misinterpreted, intentionally or unintentionally.
One such set of numbers is the newest data released on vaccination percentages broken down by age group, it also happens to give us a good sample range to conduct some statistical comparisons on.1
This isn’t for peer review so I don’t have to write a methods section, all of my sources will be listed at the end of this and I will include all pertinent tables. I am basing my death numbers off of the CDC’s “Provisional COVID-19 Deaths by Sex and Age”, all immunization data is from “National Immunization Survey Adult COVID Module (NIS-ACM): Trends in Behavioral Indicators Among Unvaccinated People”, and population data is from the US Census Bureau. Possible conflicts in comparisons made include but aren’t limited to strain variant or regional super spreader events causing anomalous deaths.
The process used was to go through the state by state data, calculate the number of COVID deaths, match that state and time period to the corresponding vaccine time period and percentage, and then look at correlation data. It is fully understood in presenting this correlation does not equal causation, but significant corollaries cannot be thrown out.2
It is also critically important to explain that I used “COVID-19 Deaths” per the CDC’s records, and is said by the CDC to be the cause of death for an individual. This will certainly miss some individuals who COVID contributed to their death but was not the principal cause of death, but if we are going to measure something we have to decide what the cutoff line is, so that was what I used, by all means, feel free to challenge my findings, email me and I will send you my data sheets and you can pick through the CDC’s very organized records and find the ones you’d like to use.
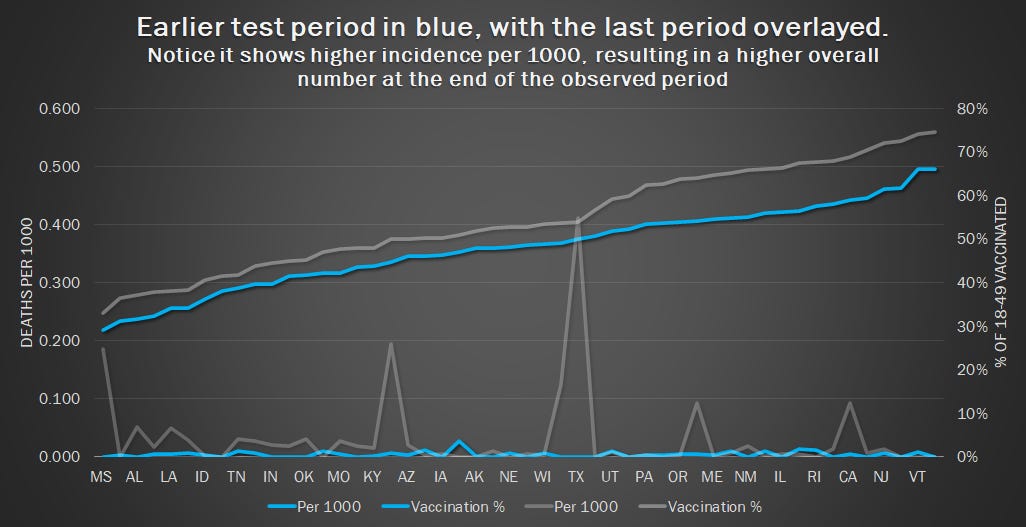
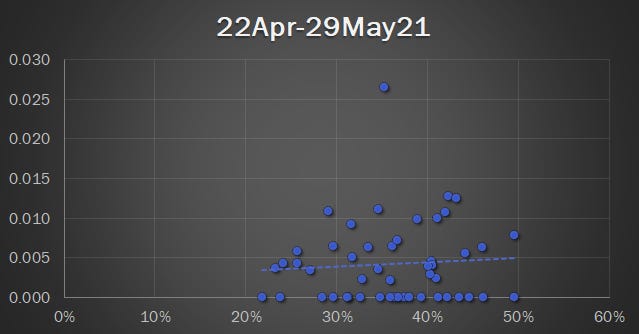
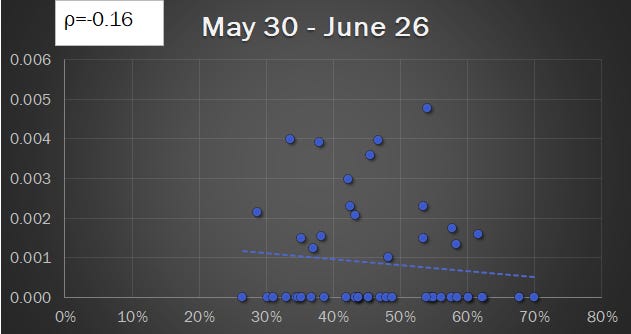
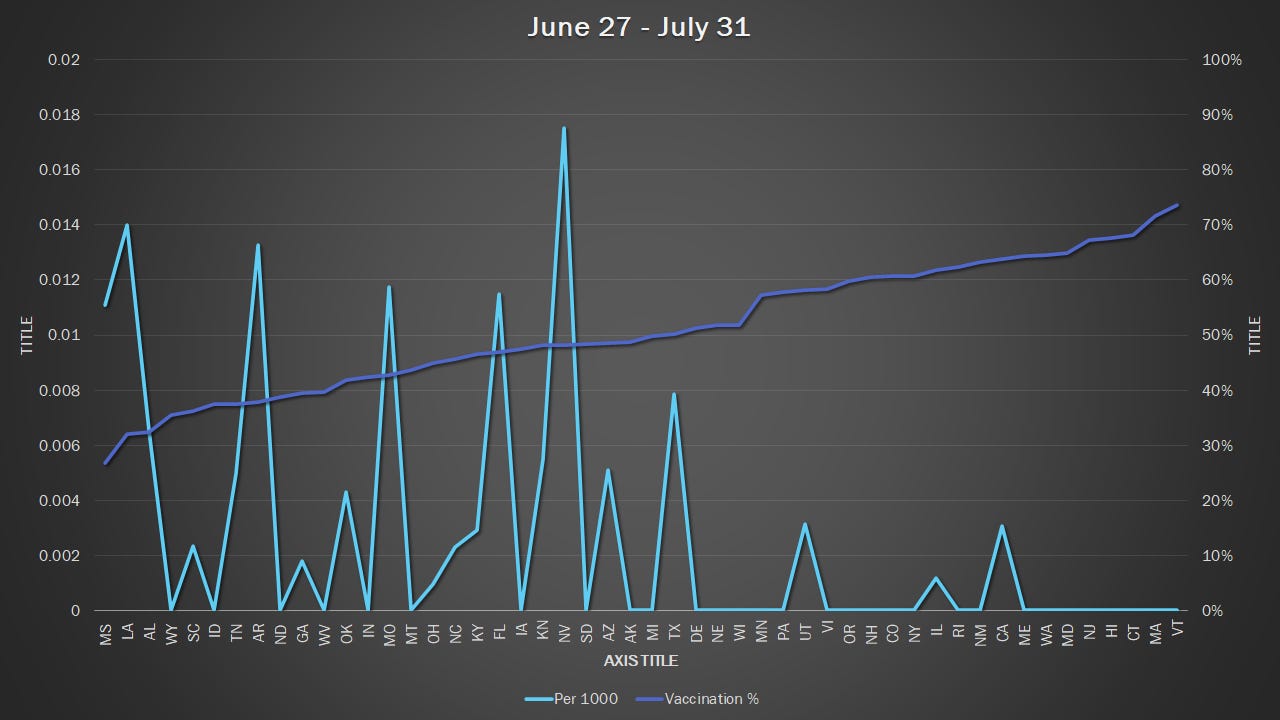
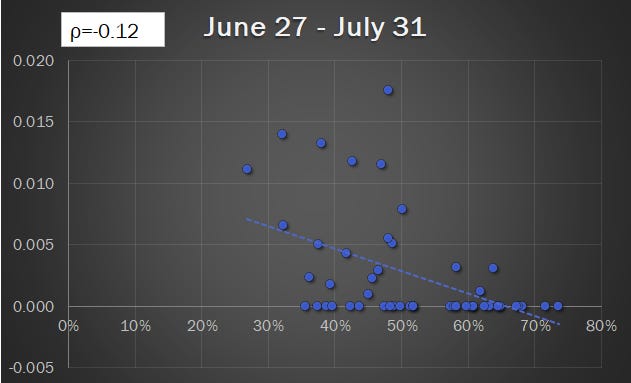
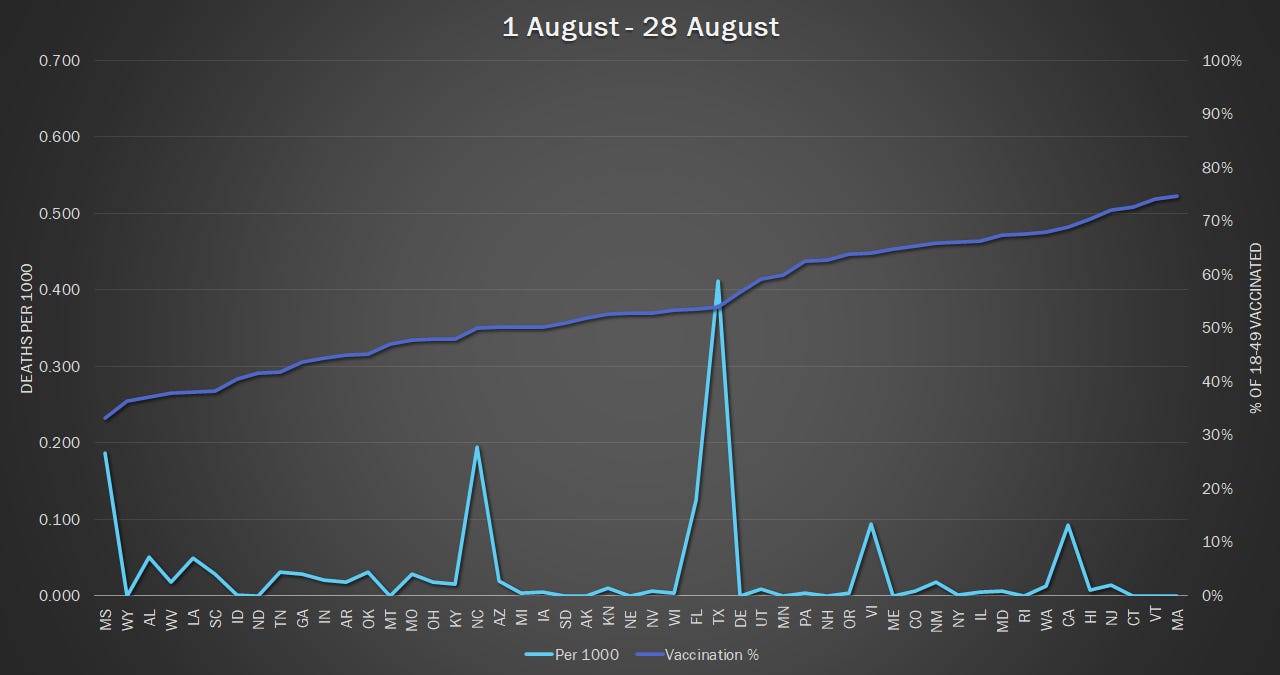
Vaccination status data and deaths were recorded in intervals of 22Apr-21May, 30May-26Jun, 27Jun-31Jul, and 01Aug-28Aug. Calculations for the 18-49 year old population were done to determine how many deaths per 1000 happened in that time frame.
Prior to doing any formal analysis, most should be able to see that there is not much connecting the lower death per million rates to vaccination rates, coupled with the drops in reproductive rates I am struggling to see how we are mandating anything other than therapy for Post Traumatic Covid Syndrome.
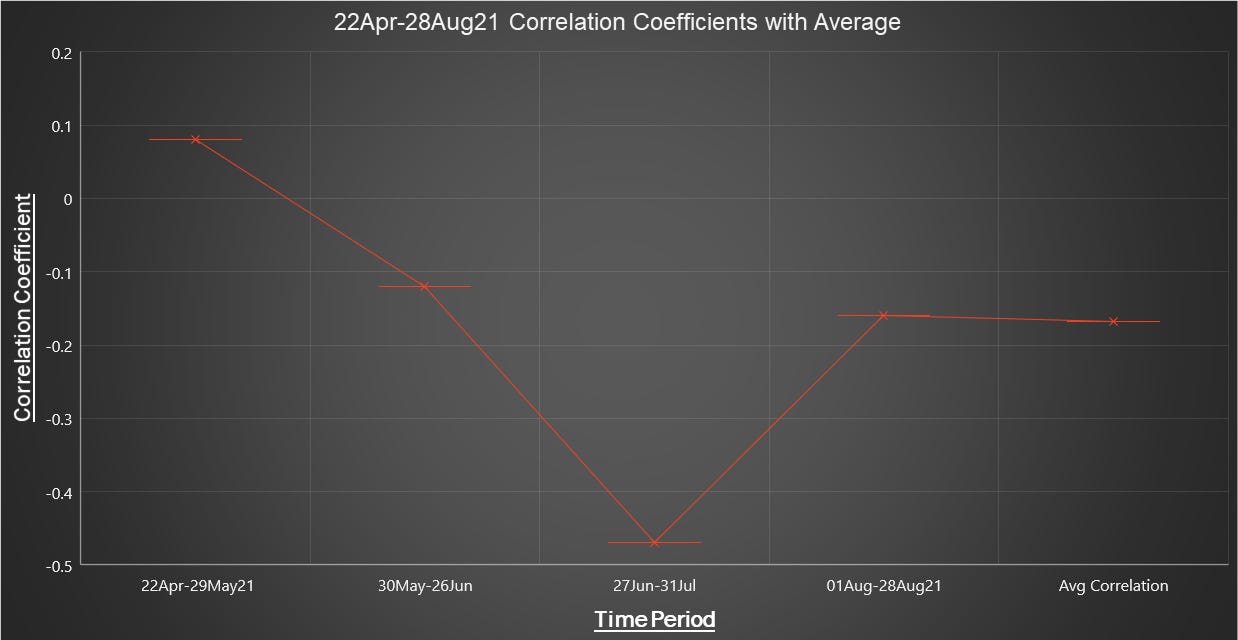
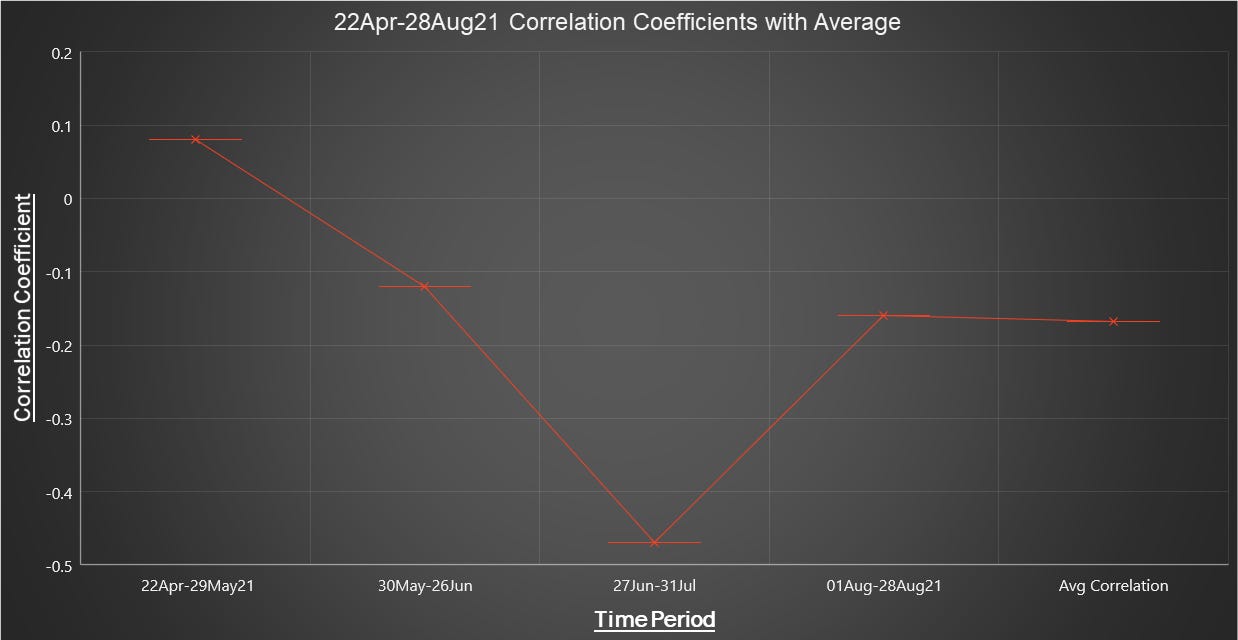
Throughout the observed period, several observations were made apparent.
The key takeaway, a negligible correlation was observed by higher rates of vaccination in a state and deaths per 1000 over periods. Meaning for roughly 1 month (average duration= 34 days) an increase in deaths per 1000 was not observed at the same time vaccination rates in all states were going up, with average vaccination rates going up 55.78% throughout the observed period. Throughout this pandemic, the largest, most emotionally charged numbers have been blasted at us by the media and leaders in this county, but unfortunately, the numbers don’t bear out the necessity for not only mandated vaccines but any of the restrictions being put on the country at this point, unless you are in a vulnerable group which military members are not. If we are requiring a drug be used on people with absolutely no idea of its long-term effects, should we not have better than, to quote the NIH “Negligible Correlation”.3 4Again, this is for an overall healthy 18-49 year old group, not only is it irresponsible to suggest action off of observational data that doesn’t seem to pan out, but we are doing it to people that don’t need it in the first place.
{kind=link}

While causality is hard to determine based on the data given due to so many contributing factors such as natural immunity, misprinting, errors such as under/over-reporting, etc; we can see what the adverse effects already being shown with the vaccine are and tell with a reasonable degree of certainty why this vaccine isn’t “just like getting the flu shot” and why it needs to be calculated in the risk assessment.



This data indicates there is no correlation between increasing vaccination rates and rates of death in the 18-49 year old population. This further indicates there is NO REASON, apart from garnering political favor, in vaccinating the force.
Part 4 discusses how it is as valid to assume the risk to military members from the vaccine is just as high if not higher than the risk of negative outcomes from contracting COVID.
“State and National Provisional Counts.” Centers for Disease Control and Prevention. Centers for Disease Control and Prevention, October 6, 2021. https://www.cdc.gov/nchs/nvss/vsrr/provisional-tables.htm.
“United States Covid-19 Cases and Deaths by State over Time.” Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. Accessed October 12, 2021. https://data.cdc.gov/Case-Surveillance/United-States-COVID-19-Cases-and-Deaths-by-State-o/9mfq-cb36.
Forgey, Quint. “Pentagon: 70 Percent of Service Members Have Received First Dose of Covid Vaccine.” POLITICO. POLITICO, July 18, 2021. https://www.politico.com/news/2021/07/16/military-coronavirus-vaccine-499822.
Ali, Zulfiqar, and S Bala Bhaskar. “Basic Statistical Tools in Research and Data Analysis.” Indian journal of anaesthesia. Medknow Publications & Media Pvt Ltd, September 2016. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5037948/.